


Pediatric dentists are the pediatricians of dentistry. A pediatric dentist has two to three years of specialty training following dental school and limits his/her practice to treating children only. Pediatric dentists are primary and specialty oral care providers for infants and children through adolescence.
Primary, or “baby,” teeth are important for many reasons. Not only do they help children speak clearly and chew naturally, they also aid in forming a path that permanent teeth can follow when they are ready to erupt.
A check-up every six months is recommended in order to prevent cavities and other dental problems. However, your pediatric dentist can tell you when and how often your child should visit based on their personal oral health.
X-rays are crucial for dental diagnostics, revealing conditions not seen in exams. They’re needed for assessing tooth eruption, bone diseases, injuries, and orthodontic planning. Early detection via X-rays makes treatment easier and more cost-effective. The American Academy of Pediatric Dentistry advises biannual X-rays for high decay risk, and yearly for most. A full set is recommended every three years. Modern dental practices ensure minimal radiation exposure with lead aprons and focused beams, making X-rays safe for children.
Tooth brushing is one of the most important tasks for good oral health. Many toothpastes, and/or tooth polishes, however, can damage young smiles. They contain harsh abrasives, which can wear away young tooth enamel. When looking for a toothpaste for your child, make sure to pick one that is recommended by the American Dental Association as shown on the box and tube. These toothpastes have undergone testing to ensure they are safe to use. Remember, children should spit out toothpaste after brushing. For ages 0 to 3 years use a smear of toothpaste, and from 3 to 6 years a small pea size.
Childhood bruxism often presents as nighttime teeth grinding, which can be stress-related or due to inner ear pressure changes. While most cases don’t need treatment, severe wear may require a mouth guard. Risks include choking and potential jaw growth interference. Fortunately, bruxism typically diminishes by age 6-9 and usually ends by age 9-12. Consult a pediatrician or dentist if concerned.
- Toothache: Persistent pain in your mouth without any apparent cause.
- Sensitivity: A mild to sharp pain when eating or drinking something sweet, hot, or cold.
- Visible Holes or Pits: Small openings or holes in your teeth.
- Stains: Brown, black, or white staining on any surface of a tooth.
- Pain When Biting: Discomfort or pain when you bite down.
If your child complains of any unusual tooth sensations or you see these visible signs of decay, call the office right away to schedule a dental exam.
For any treatment that might cause pain, the area is numbed with a local anesthetic, then an injection with a stronger local anesthetic is used. The child won’t feel any pain but may feel pressure around the area. If the child has any dental anxiety our office also uses nitrous oxide (“laughing gas”) to help them relax.
- Immediately following the extraction, keep closed on gauze at the extraction site for a blood clot to form.
- Don’t drink anything warmer than room temperature for a few hours after the extraction.
- Chew on the other side of the mouth.
- Avoid physical exertion for a few days.
- Do not use any straws, and avoid spitting.
- Avoid foods that are crunchy, spicy, or acidic (tomato or vinegar-based dishes, so neither Western nor Eastern Carolina BBQ).
- Some foods you can eat would include mac and cheese, white sauce pasta dishes, steamed vegetables, ice cream, coleslaw (non-vinegar based) etc. You should also receive an aftercare sheet at the office with instructions on care for an extraction.
Developing malocclusions, or bad bites, can be recognized as early as 2-3 years of age. Often, early steps can be taken to reduce the need for major orthodontic treatment at a later age.
- Stage I – Early Treatment: This period of treatment encompasses ages 2 to 6 years. At this young age, we are concerned with underdeveloped dental arches, the premature loss of primary teeth, and harmful habits such as finger or thumb sucking. Treatment initiated in this stage of development is often very successful and many times, though not always, can eliminate the need for future orthodontic/orthopedic treatment.
- Stage II – Mixed Dentition: This period covers the ages of 6 to 12 years, with the eruption of the permanent incisor (front) teeth and 6-year molars. Treatment concerns deal with jaw malrelationships and dental realignment problems. This is an excellent stage to start treatment, when indicated, as your child’s hard and soft tissues are usually very responsive to orthodontic or orthopedic forces.
- Stage III – Adolescent Dentition: This stage deals with the permanent teeth and the development of the final bite relationship.

This is a very common occurrence with children, usually the result of a lower, primary (baby) tooth not falling out when the permanent tooth is coming in. In most cases, if the child starts wiggling the baby tooth, it will usually fall out on its own within two months. If it doesn’t, then contact your pediatric dentist, where they can easily remove the tooth. The permanent tooth should then slide into the proper place.
When a child begins to participate in recreational activities and organized sports, injuries can occur. A properly fitted mouth guard, or mouth protector, is an important piece of athletic gear that can help protect your child’s smile, and should be used during any activity that could result in a blow to the face or mouth. Mouth guards help prevent broken teeth, and injuries to the lips, tongue, face, or jaw. A properly fitted mouth guard will stay in place while your child is wearing it, making it easy for them to talk and breathe. Ask your pediatric dental care provider about custom and store-bought mouth protectors.
We recommend that you make an appointment to see the dentist as soon as your child gets their first tooth. The American Academy of Pediatric Dentistry recommends that children be seen after their first tooth erupts, or at one year of age, whichever comes first.
The first visit is usually short and simple. In most cases, we focus on getting to know your child and giving you some basic information about dental care. The doctor will check your child’s teeth for placement and health, and will look for any potential problems with the gums and jaw. If necessary, we may do a bit of cleaning. We will also answer any questions you have about how to care for your child’s teeth as they develop, and provide you with materials containing helpful tips that you can refer to at home.
The American Academy of Pediatric Dentistry (AAPD) recommends that all pregnant women receive oral healthcare and counseling during pregnancy. Research has shown evidence that periodontal disease can increase the risk of preterm birth and low birth weight. Talk to your doctor or dentist about ways you can prevent periodontal disease during pregnancy. Additionally, mothers with poor oral health may be at a greater risk of passing the bacteria which causes cavities to their young children. Mothers should follow these simple steps to decrease the risk of spreading cavity-causing bacteria:
- Visit your dentist regularly.
- Brush and floss on a daily basis to reduce bacterial plaque.
- Proper diet, with the reduction of beverages and foods high in sugar & starch.
- Use a fluoridated toothpaste recommended by the ADA and rinse every night with an alcohol-free, over-the-counter mouth rinse with 0.05% sodium fluoride to reduce plaque levels.
- Don’t share utensils, cups, or food which can cause the transmission of cavity-causing bacteria to your children.
- Use of xylitol chewing gum (4 pieces per day by the mother) can decrease a child’s cavity rate.
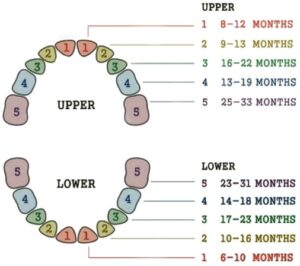
The first primary (or baby) teeth to erupt through the gums are the lower central incisors, as early as 4 months, followed closely by the upper central incisors. Although all 20 primary teeth usually appear by age 3, the pace and order of their eruption varies. Permanent teeth begin appearing around age 6, starting with the first molars and lower central incisors.
Baby Bottle Tooth Decay – One serious form of decay among young children is baby bottle tooth decay. This condition is caused by frequent and long exposures of an infant’s teeth to liquids that contain sugar. Among these liquids are milk (including breast milk), formula, fruit juice, and other sweetened drinks.
Putting a baby to bed for a nap or at night with a bottle other than water can cause serious and rapid tooth decay. Sweet liquid pools around the child’s teeth giving plaque bacteria an opportunity to produce acids that attack tooth enamel. If you must give the baby a bottle as a comforter at bedtime, it should contain only water. If your child won’t fall asleep without the bottle and its usual beverage, gradually dilute the bottle’s contents with water over a period of two to three weeks.
After each feeding, wipe the baby’s gums and teeth with a damp washcloth or gauze pad to remove plaque. The easiest way to do this is to sit down, place the child’s head in your lap or lay the child on a dressing table or the floor. Whatever position you use, be sure you can see into the child’s mouth easily.
Sippy cups should be used as a training tool from the bottle to a cup and should be discontinued by the first birthday. If your child uses a sippy cup throughout the day, fill the sippy cup with water only (except at mealtimes). By filling the sippy cup with liquids that contain sugar (including milk, fruit juice, sports drinks, etc.) and allowing a child to drink from it throughout the day, it soaks the child’s teeth in cavity-causing bacteria.
Thumb and pacifier sucking habits will generally only become a problem if they go on for a very long period of time. The earlier a child can stop a sucking habit, the less chance there is that it will lead to orthodontic problems down the road. Most children stop these habits on their own, but if they are still sucking their thumbs or fingers past the age of three, a mouth appliance may be recommended by your pediatric dentist.
Parents should use a tiny smear or rice size of fluoride toothpaste to brush baby teeth twice daily as soon as they erupt to 3 years of age. Once children are 3 to 6 years old, then the amount should be increased to a pea-size dollop and perform or assist your child’s toothbrushing. Use a soft bristle, age-appropriate sized toothbrush. Remember that young children do not have the ability to brush their teeth effectively so they will need your help. Children should spit out and not swallow excess toothpaste after brushing.
